Reactive Histiocytosis in a Dog: Differentials, Possible Treatments, and Other Considerations
Jeremie Korchia, DVM, MS, DACVP
A 9-year-old intact, female, cross breed dog was presented to a practitioner for subcutaneous masses all over the body. A fine needle aspirate of one mass was submitted to the Texas A&M Veterinary Medical Diagnostic Laboratory (TVMDL). It was highly cellular and mostly consisted of atypical round/hemic cells distributed individually within a large amount of blood (Figures 1 and 2 below). Cells had moderate amounts of moderately basophilic cytoplasm, and contained small numbers of small vacuoles. Anisocytosis and anisokaryosis were moderate. Nuclei were round to slightly ovoid and eccentric and had finely stippled chromatin with 2 to 3 intermediate, indistinct nucleoli. Binucleation was mild, and mitotic figures were present in small numbers. The cytologic interpretation was round cell proliferation with moderate atypia. The morphological appearance was highly supportive for a histiocytic lineage. In this clinical context, the most likely differential was a reactive histiocytosis. However, other histiocytic diseases could not be completely ruled out.
Cutaneous histiocytic proliferations in dogs have several differentials varying in terms of:
- Process: reactive or neoplastic
- Cell of origin: Interstitial dendritic cell (IDC), Langerhans cell (LC), or macrophages (not expected as the differential for cutaneous proliferations)
- Immunohistolabeling: directly function of the cell of origin, usually regardless of the pathologic process
- Therapeutic management
There are two primary differentials for a cutaneous histiocytic proliferation with numerous cutaneous/subcutaneous masses in dogs. The most frequent differential is cutaneous reactive histiocytosis, a disease that starts in the interstitial dendritic cell (IDC) and has a reactive pathologic process. The second disease, cutaneous Langerhans cell histiocytosis, is much rarer. Starting in the Langerhans cell (LC), its pathologic process is considered neoplastic.
Other histiocytic proliferations in dogs usually present as a single mass, but can sometimes present as limited numbers of masses, too. Examples of these proliferations is histiocytoma, which begins in the LC and has a neoplastic benign pathologic process, and disseminated histiocytic sarcoma, which begins in the IDC and has a neoplastic malignant pathologic process.
In the aforementioned case, the most likely diagnosis corresponded with a cutaneous reactive histiocytosis. For this diagnosis, confirmation could be obtained by histopathology combined with proper immunohistolabeling:
- Cells are expected positive for: CD204, Thy1 (CD90), MHCII, CD1a, CD4, CD18, and CD11c
- Cells are expected negative for: CD11d and ECad
The main differentials for the reactive histiocytosis (from IDC) correspond with diseases from LC, therefore, if finances are limited, confirmation can be obtained by the following:
- Thy 1 (specific for IDC)
- CD204 (positive in IDC, negative in LC)
- Ecad (specific for LC)
In the presence of a cutaneous reactive histiocytosis, a systemic reactive histiocytosis, which is the equivalent of cutaneous reactive histiocytosis that affects internal organs, cannot be completely ruled out. In that case, lymph nodes, mucosa, and/or internal organs would be affected as well.
Finally, the therapeutic management varies broadly between the different differentials, emphasizing the critical importance of reaching an accurate diagnosis. Few scientific sources are available concerning the best medical management of cutaneous reactive histiocytosis in dogs, and recommendations vary depending on sources. For example, some recommend Cyclosporine A (Affolter, Moore, Dermatopathol, 2000), whereas others recommend the combination of tetracycline/niacinamide (Palmeiro, Morris, Goldschmidt, Mauldin, 2007).
Histiocytomas are expected to be definitely cured by simple surgical excision, and may even heal spontaneously with time due to a local lymphoid response. The treatment for Langerhans cell histiocytosis may include corticosteroids and chemotherapy.
Thus, further diagnostic investigation, and consultation with an internist or an oncologist is encouraged. TVMDL offers consultation services on various cytological cases in addition to an array of clinical pathology test offerings. To learn more about diagnostic testing and services, visit tvmdl.tamu.edu or call one of our full-service laboratories in College Station or Amarillo. For more information on this case, contact Dr. Jeremie Korchia at 1.888.646.5623.
References
Affolter VK, Moore PF. Am J Dermatopathol. 2000 Feb;22(1):40-8
Palmeiro BS, Morris DO, Goldschmidt MH, Mauldin EA. Vet Dermatol. 2007 Oct;18(5):332-40
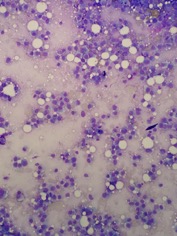
Figure 1: Fine needle aspirate from a subcutaneous mass showing a histiocytic proliferation with moderate atypia. Magnified 20x.
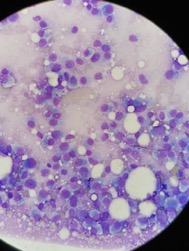
Figure 2: Photomicrograph magnified 50x depicting a subcutaneous mass interpreted as most likely cutaneous reactive histiocytosis in a clinical context of multiple cutaneous mass all over the body.